Table of contents
The recent March 2026 verdict by the Supreme Court of India in the Harish Rana case marks a significant milestone in India’s legal and ethical journey regarding the "Right to Die with Dignity."
For a UPSC aspirant, this topic intersects:
- GS Paper II: Government policies, welfare schemes, judiciary
- GS Paper IV: Ethics — right to life, dignity, medical ethics, end-of-life care
- Essay Paper: Dignity in death, medical intervention vs. natural death, state vs. individual rights
- Prelims: Landmark SC judgments, constitutional provisions (Article 21)
1. CONTEXT: THE HARISH RANA VERDICT (MARCH 2026)
On March 12, 2026, the Supreme Court of India — in a landmark 286-page judgment — permitted the withdrawal of life-sustaining treatment for 32-year-old Harish Rana, who had been in a Persistent Vegetative State (PVS) for nearly 13 years following a fall from the fourth floor of his paying guest accommodation in 2013.

| Bench | Justices J.B. Pardiwala and K.V. Viswanathan |
| Key Direction | Withdrawal of CANH from Harish Rana; AIIMS Delhi directed to shift him to a palliative care centre |
| Significance | First Indian court order approving passive euthanasia under the SC's own 2018 constitutional framework |
| Waiver Granted | The usual 30-day reconsideration (cooling-off) window was waived, as both medical boards found the condition irreversible |
The court noted that the family had "left no stone unturned" to care for Harish, and that only when the matter reached a "point of no return" did they resort to this legal route. The bench observed: "Our decision today does not neatly fit within logic and reason alone. It sits in a space between love, loss, medicine and mercy."
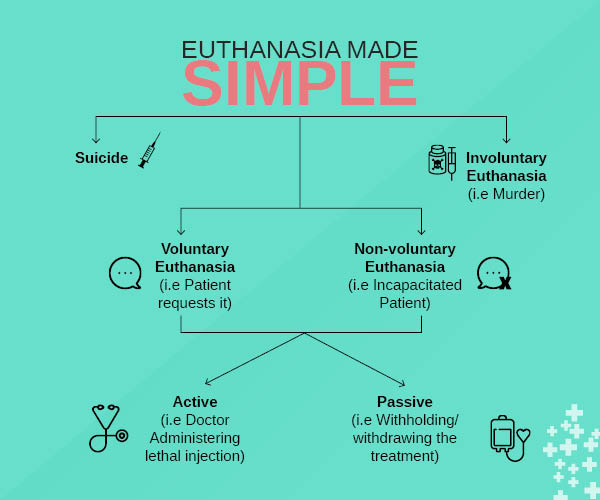
2. ACTIVE VS. PASSIVE EUTHANASIA
2.1 Euthanasia — Definition
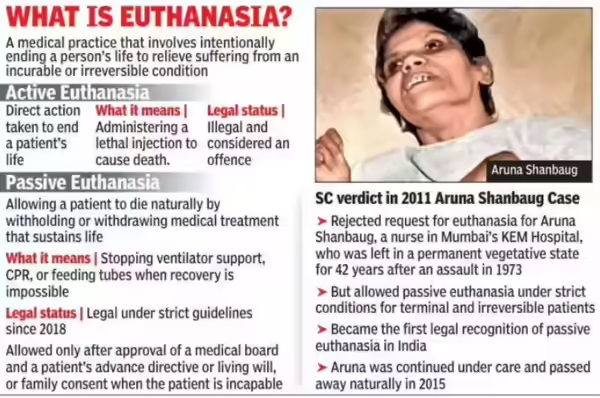
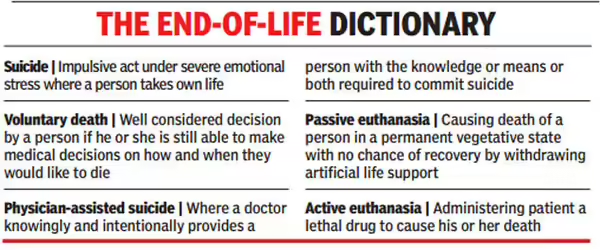
Euthanasia refers to the deliberate ending of a person's life to relieve intractable suffering. The term derives from the Greek words eu (good) and thanatos (death).
2.2 Active Euthanasia
Active euthanasia involves intentionally causing death through a positive, overt act — such as the administration of a lethal injection or drug.
- Introduces a new, external agency of harm that directly causes death
- Death is not a result of the underlying illness but of an intervention that sets a new chain of events in motion
- Legal in countries such as the Netherlands, Belgium, Canada (limited cases), and some US states
- Illegal in India — amounts to culpable homicide under the Bharatiya Nyaya Sanhita (BNS)
- A doctor assisting in such an act faces criminal liability for abetment to suicide
2.3 Passive Euthanasia
Passive euthanasia involves withdrawing or withholding medical treatment that is artificially prolonging life, allowing the underlying fatal condition to take its natural course.
- Does NOT introduce a new cause of death — the doctor does not create a new risk
- The physician is "allowing death to occur", not causing it
- The patient's affliction is due to factors independent of the doctor
- Permissible in India under strict conditions laid down by the Supreme Court.
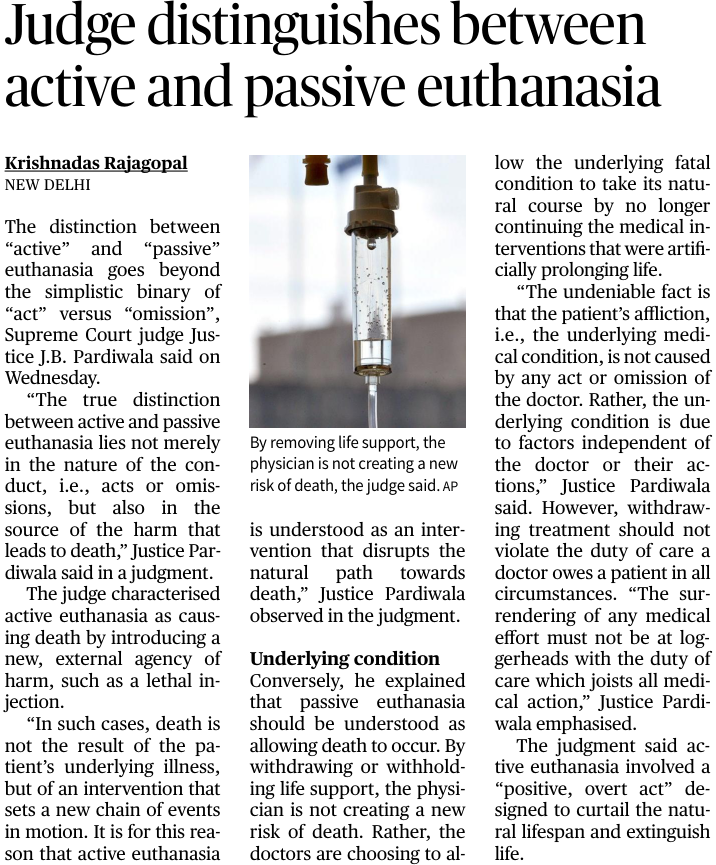
2.4 Justice Pardiwala's Distinction — Beyond Act vs. Omission
Traditionally, active euthanasia is characterised as an "act" and passive euthanasia as an "omission". However, Justice Pardiwala clarified that this is an oversimplification. The true distinction lies in the source of the harm that leads to death:
- Active euthanasia: harm comes from an introduced external agency (the lethal act itself)
- Passive euthanasia: harm flows from the patient's own underlying condition; the doctor merely stops an artificial impediment to natural death
- Withdrawing treatment should not violate the duty of care a doctor owes a patient in all circumstances
- The surrendering of medical effort must not be "at loggerheads with the duty of care which joists all medical action"
KEY DISTINCTION FOR MAINS:
- Active euthanasia = introducing new cause of death (illegal in India)
- Passive euthanasia = removing artificial life support, allowing natural death (permitted under SC guidelines)
- The difference lies not merely in act vs. omission, but in the SOURCE of the causal harm
- CANH (Clinically Assisted Nutrition & Hydration) = medically supervised treatment, NOT ordinary feeding
3. CONSTITUTIONAL & LEGAL FRAMEWORK
3.1 Article 21: Right to Life and Personal Liberty
Article 21 guarantees that no person shall be deprived of their life or personal liberty except according to a procedure established by law. The SC has progressively expanded this to include:
- Right to live with human dignity (Maneka Gandhi v. Union of India, 1978)
- Right to health and medical care
- Right to die with dignity — the central question in euthanasia jurisprudence
3.2 Evolution: Right to Die as Part of Right to Live with Dignity
For terminally ill or persistently vegetative patients whose life is "ebbing out", the SC has held that the Constitution protects the choice not to be kept alive through invasive or futile medical intervention. When death due to the termination of natural life is "certain and imminent and the process of natural death has commenced", a premature end to life may fall within the ambit of the right to die with dignity.
3.3 The Law on Attempted Suicide
While Section 309 of the IPC (now BNS) criminalises attempted suicide, the SC has repeatedly observed that a person attempting suicide requires care, not punishment. Doctors assisting patients in performing the act face criminal liability for abetment — a distinction crucial to the euthanasia debate.
3.4 No Comprehensive Legislation
India has no legislation governing euthanasia or end-of-life care. The SC bench pointedly observed: "There are moments when legislative inaction speaks more loudly than legislative action."

4. TIMELINE: KEY JUDICIAL MILESTONES
| Year / Case | Key Development |
|---|---|
| 2011 — Aruna Shanbaug v. Union of India | SC held that passive euthanasia cases would need to be approved by the High Court. Aruna Shanbaug, a nurse at Mumbai's KEM Hospital, sexually assaulted in 1973, remained in a vegetative state for decades. Nurses who cared for her opposed withdrawal of treatment. |
| 2018 — Common Cause v. Union of India | Constitution Bench held that the right to die with dignity is an inseparable facet of Article 21. Recognised Advance Medical Directives (Living Wills). Allowed two medical boards to take the decision with consent of next of kin. Also classified CANH as a medical treatment, not ordinary feeding. |
| 2018 — Safeguards & Guidelines | Advance directives to be attested before a notary or gazetted officer and stored in digital health records. Required signing by two witnesses and countersigning by a judicial magistrate. |
| 2023 — Simplified Guidelines | Court acknowledged "insurmountable obstacles" in the 2018 framework. Removed mandatory Collector's role; two medical boards can now take the decision; magistrate must be informed but approval no longer required. |
| March 2026 — Harish Rana Case | First actual court order applying the passive euthanasia framework. SC permitted withdrawal of CANH. Described CANH as a "technologically mediated medical intervention". Waived the 30-day cooling-off period. Directed AIIMS Delhi to shift Rana to a palliative care centre. |
5. THE PROCEDURE FOR PASSIVE EUTHANASIA (2023 GUIDELINES)
The Union Health Ministry released draft guidelines in 2024, based on the court's 2023 directives:
Step 1 — Treating Physician's Assessment The treating physician must decide whether the patient has any hope of recovery or a good quality of life if treatment measures remain in place.
Step 2 — Primary Medical Board A primary board assesses the case and reaches a consensus. It comprises the treating physician and two subject experts with five or more years of experience.
Step 3 — Family Discussion Doctors must discuss the prognosis with the family and ascertain whether they want any other treatment. A shared decision must be taken; the team must produce a consistent plan for care.
Step 4 — Secondary Medical Board (if withdrawal is sought) Consists of:
- A doctor nominated by the Chief Medical Officer (CMO) of the district
- Two subject experts with five or more years of experience
- The board must take a decision within 48 hours
Hospitals must also inform the Magistrate before withdrawal of treatment. However, the Magistrate's approval is no longer required — only notification.
PRACTICAL HURDLES (Important for Mains):
- Insufficient doctors with expertise across all hospitals
- Very few states have created the Secondary Medical Board (Maharashtra, Goa, Karnataka are exceptions)
- CMOs must send nomination lists — many have not done so
- Private hospitals are reluctant due to fear of litigation
- High guilt burden on families; difficult to find willing doctors
- Advance Directives remain largely unused due to lack of awareness

6. CLINICALLY ASSISTED NUTRITION & HYDRATION (CANH)
| What is CANH? | Administration of nutrition and fluids through medical means (e.g., feeding tubes, IV drip), as opposed to natural eating and drinking |
| SC's Finding (2026) | CANH is a "medically supervised treatment" — not ordinary feeding. It is "prescribed, supervised and periodically reviewed by trained healthcare professionals in accordance with established medical standards" |
| Why This Matters | Since CANH = medical treatment, discontinuing it = withdrawing medical treatment (permitted), NOT starving the patient (which would be illegal) |
| Delhi HC's Earlier Error | Delhi HC had said Rana was not dependent on mechanical life support since he could breathe on his own. SC disagreed — artificial feeding via CANH requires clinical judgment and cannot be equated with ordinary feeding |
7. ADVANCE DIRECTIVES / LIVING WILLS
7.1 What Can a Living Will Do?
- Specify the type of care the person would like to receive
- Specify the gender by which the person would like to be addressed
- Nominate a person (who may be someone other than a family member) to take medical decisions on their behalf
- Refuse specific life-prolonging interventions (e.g., CPR, ventilator support, dialysis, chemotherapy, radiotherapy)
7.2 How to Create One (Post-2023 Rules)
- Attest before a notary or gazetted officer
- Signed by two witnesses
- Can be stored in digital health records
- Collector's role and hospital board no longer mandatory for attestation
7.3 Significance
Living wills ease the process by making the patient's wishes known through a legally enforceable document. This reduces the moral and emotional burden on families and provides clearer legal protection to doctors who follow them.
8. RIGHT TO DIGNIFIED DEATH VS. STATE INTEREST IN PRESERVING LIFE
8.1 The State's Interest
Traditionally, the state has an absolute interest in preserving life. This flows from the sovereign duty to protect citizens and the principle of sanctity of life. However, the SC held that this interest is not unconditional.
8.2 The Tipping Point Principle
Justice Pardiwala articulated a crucial principle: the state's absolute interest in preserving life must become subservient to a patient's right to dignity at a "tipping point" — when medical interventions become increasingly futile and invasive while the chances of recovery keep dropping.
"When the degree of bodily invasion progressively increases, and the prognosis for recovery progressively decreases, there arises a certain point when the state's absolute interest in preserving life must become subservient to the dignity of the individual, though he is unconscious or incompetent."
Keeping a terminally ill patient alive solely because technology permits it — compelling them to endure a slow, agonising death — "cannot fully be compatible with the Constitutional ideal of dignity."
8.3 Dignity as the Most Sacred Possession
The court reaffirmed that dignity is the most sacred possession of a human being. Its possession "can neither be said to lose its sanctity in the process of death nor when death occurs." The interest of the state must not be allowed to overpower the dignity which must be equally assured to individuals in the process of life and death.
IMPORTANT QUOTES FOR ESSAY/MAINS:
- "This decision is not about choosing death, but is rather one of not artificially prolonging life." — Justice Pardiwala
- "Dignity is the most sacred possession of a human being. Its possession can neither be said to lose its sanctity in the process of death nor when death occurs." — Justice Pardiwala
- "This decision can feel like an act of surrender, but we believe it is, in truth, an act of profound compassion and courage." — Justice Pardiwala (to Harish Rana's family)
9. ETHICAL DIMENSIONS (GS Paper IV)
9.1 Arguments FOR Passive Euthanasia
- Respect for Autonomy: Individuals have the right to decide what happens to their own bodies, including refusing futile treatment
- Human Dignity: Forcing an irreversible condition to continue through artificial means is an affront to dignity
- Prevention of Suffering: Prolonging a vegetative state does not benefit the patient — it may extend suffering
- Resource Allocation: Medical resources used to prolong futile lives could serve patients who can genuinely benefit
- Family Well-being: Prolonged PVS causes severe emotional and financial burden on families
9.2 Arguments AGAINST / Concerns
- Sanctity of Life: Many religious and ethical traditions hold that life is sacred and should not be ended deliberately
- Slippery Slope: Permitting passive euthanasia may open the door to active euthanasia and abuse
- Diagnostic Uncertainty: PVS can sometimes be misdiagnosed; rare recoveries have occurred
- Potential for Abuse: Vulnerable patients could be pressured by families or institutions for financial reasons
- Duty of Care: Medicine's core principle — primum non nocere (first, do no harm) — may be in tension with withdrawal
9.3 Ethical Frameworks at Play
| Framework | Application |
|---|---|
| Consequentialism | Withdrawal is justified if it reduces overall suffering and serves the best interest of the patient |
| Deontology | Tension: duty to respect patient autonomy vs. duty not to take life |
| Virtue Ethics | What would a compassionate and reasonable doctor/family do? The SC explicitly invoked compassion and courage |
| Care Ethics | Emphasises relationships — the family's years of devotion and the court's acknowledgment of their love are central |
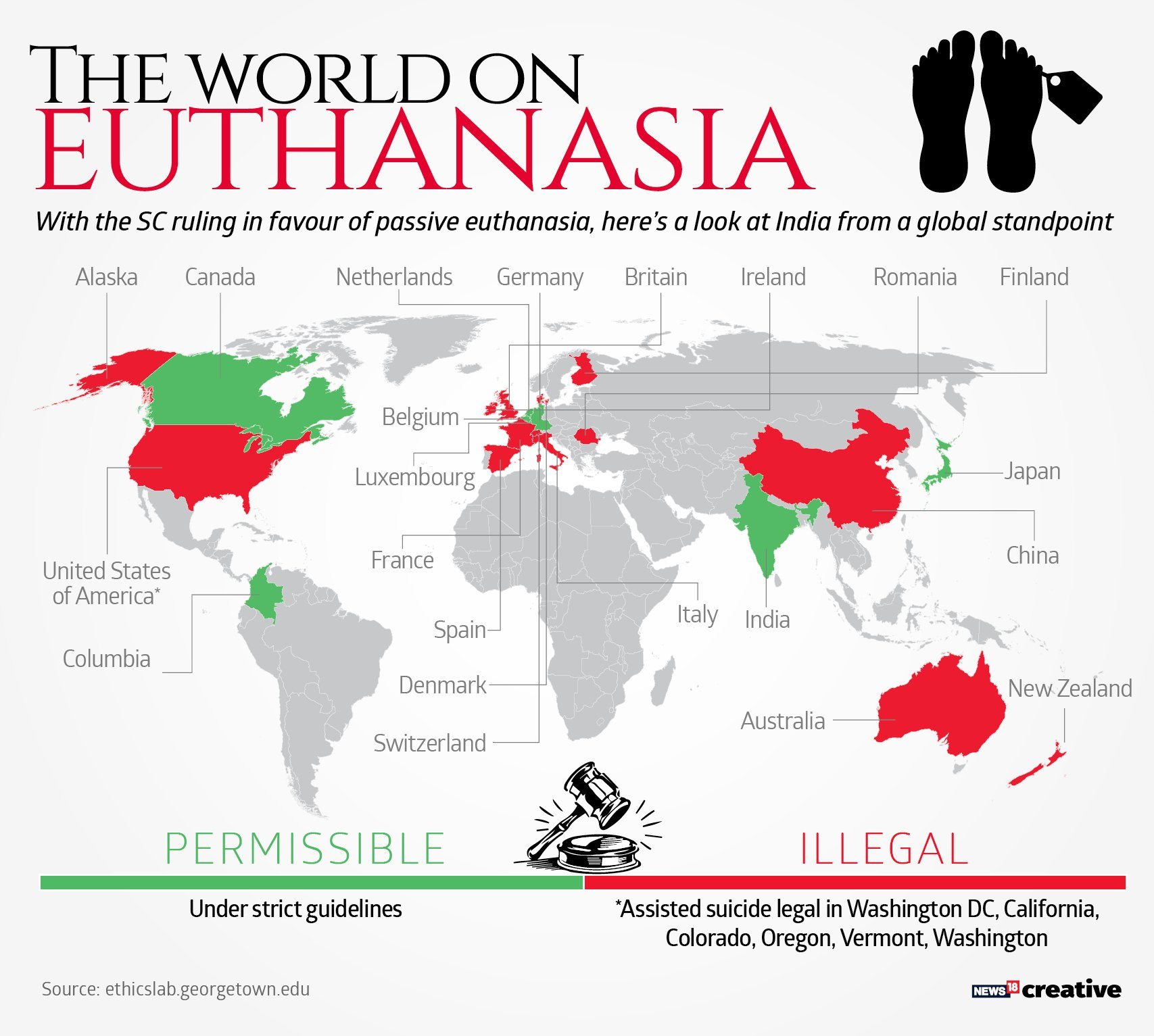
10. GLOBAL COMPARATIVE PERSPECTIVE
| Country | Framework |
|---|---|
| Netherlands & Belgium | Both active and passive euthanasia permitted under strict conditions (terminal illness, unbearable suffering, voluntary and repeated request) |
| Canada | Medical Assistance in Dying (MAID) permitted since 2016; expanded in 2021 to include non-terminal illness cases |
| USA | Death with Dignity Acts in Oregon (1997) and several states allow physician-assisted suicide; passive euthanasia generally permitted |
| UK | Active euthanasia and assisted dying remain illegal; passive euthanasia allowed under careful clinical and judicial oversight |
| India | Active euthanasia illegal; passive euthanasia permitted under SC guidelines (no legislation); first approved case: Harish Rana (2026) |
| Switzerland | Assisted suicide legal; basis for "suicide tourism" — foreigners travel to Switzerland for end-of-life assistance |
11. WAY FORWARD AND POLICY RECOMMENDATIONS
11.1 Legislation
- Parliament must enact a comprehensive end-of-life care law to replace the current judge-made framework
- Clear definitions, procedural safeguards, and liability protections for doctors are essential
11.2 Institutional Strengthening
- All states must constitute Secondary Medical Boards with empanelled, qualified nominated doctors
- CMOs must send updated nomination lists — currently a major bottleneck
- Training programmes for doctors in palliative care and end-of-life communication
11.3 Awareness and Living Wills
- Public awareness campaigns on the right to create Advance Medical Directives
- Integration of living will registration with digital health records under ABDM/ABHA
- Hospitals should proactively inform patients of their right to create living wills
11.4 Palliative Care Expansion
- India's palliative care infrastructure is extremely limited — needs urgent expansion
- Withdrawal of life support must be firmly tied to robust palliative care (as directed by the SC)
11.5 Reducing Litigation Fear
- Legal protection and safe-harbour provisions for doctors who follow prescribed procedures in good faith
- Private hospitals need clear guidelines and protection so they are not deterred from following the law
12. QUICK FACTS FOR PRELIMS
- Article 21: Right to Life — expanded by SC to include right to die with dignity
- Aruna Shanbaug Case (2011): First SC judgment on passive euthanasia; required HC approval
- Common Cause Case (2018): Constitution Bench — recognised living wills; two medical boards
- 2023 SC Guidelines: Simplified process; no HC approval; notary attestation sufficient for living wills
- Harish Rana (2026): First actual SC order approving passive euthanasia
- CANH = Clinically Assisted Nutrition and Hydration — classified as medical treatment by SC
- Secondary Medical Board: Doctor from CMO list + 2 subject experts; must decide in 48 hours
- Magistrate Role (post-2023): Must be informed, but approval not required
- Active Euthanasia: Illegal in India; lethal injection/act = new external cause of death
- Passive Euthanasia: Legal under SC guidelines; no legislation yet passed by Parliament
- PVS = Persistent Vegetative State — unconscious but with preserved brainstem functions
- BNS (Bharatiya Nyaya Sanhita): Replaced IPC; active euthanasia = culpable homicide
13. CONCLUSION
The Supreme Court's order in the Harish Rana case is a watershed moment in Indian legal history. For the first time, India's highest court has moved from articulating a framework for passive euthanasia to actually applying it — giving judicial sanction to a family's painful but compassionate decision to let their loved one go.
The verdict reaffirms that the right to life under Article 21 is not merely a right to biological survival, but a right to live — and ultimately die — with dignity. It places human dignity at the centre of end-of-life care, above the state's paternalistic interest in preserving life at any cost.
Yet the judgment also lays bare the institutional and legislative gap: India still has no law on euthanasia. What is now needed is a comprehensive legal framework, robust palliative care infrastructure, and a cultural shift in how India approaches death, dying, and dignity.
